

The Gap Nobody Wants to Talk About

Dr. Chokshi calls it the “discovery-delivery gap” — or more bluntly, the “no-do gap.” It’s the distance between what medicine already knows works and what patients actually receive.
This isn’t a fringe problem. Half of patients with high blood pressure aren’t controlled. Curative medicines for conditions like hepatitis C exist right now but don’t reach the people who need them most. HIV prevention tools with near-perfect efficacy in clinical trials sit underutilized in the communities carrying the highest burden of disease.
The science isn’t failing. The system is.
That distinction matters enormously when you’re deciding where to direct AI investment, clinical attention, and public health infrastructure. Chasing the next breakthrough while ignoring delivery failures isn’t progress — it’s distraction.
What “Closing the Gap” Actually Looks Like
So where does AI fit? Dr. Chokshi points to two concrete, underappreciated functions.
Case Finding at Scale

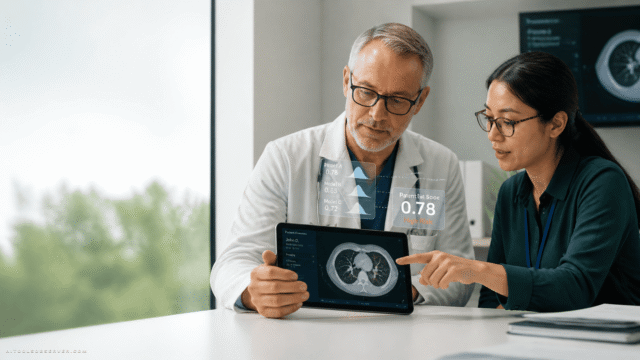
The first is augmenting case finding — using AI to surface patients who have an undiagnosed condition, qualify for a proven intervention, or have quietly fallen out of care before completing treatment.
“We know how to control blood pressure. This is not rocket science. We don’t need AI to tell us what to do about that,” Dr. Chokshi said. “But AI can help through doing things like augmenting our case finding.”
This is AI doing something genuinely useful: not replacing clinical judgment, but extending its reach. Identifying the person with undiagnosed hepatitis C before they develop cirrhosis. Flagging the hypertensive patient who missed their last three appointments. Connecting people to care that already works, faster and more reliably than fragmented systems currently allow.
Navigation Through the Handoffs

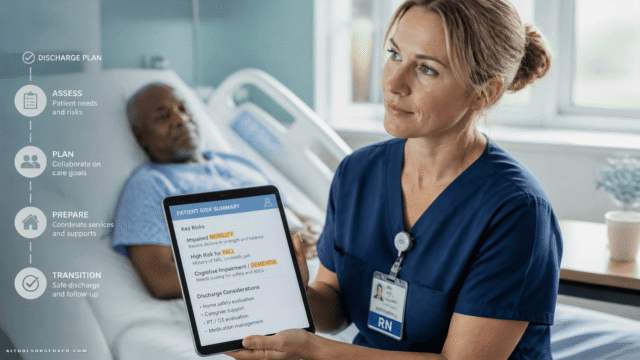
The second function is navigation — helping patients move from diagnosis through the full arc of treatment. Scheduling. Prior authorization. Follow-up. Completion of care.
That’s where healthcare systems lose people. Not because the science is wrong, but because the process is exhausting, fragmented, and indifferent to patients’ real lives.
AI deployed here isn’t a flashy innovation. It’s infrastructure for follow-through. And Dr. Chokshi is direct about why that matters: “How do we direct AI, not just to the breakthroughs, but to the follow-throughs?”
The Equity Dimension You Can’t Ignore

Here’s where the stakes get higher.
If AI in healthcare is primarily aimed at making already-efficient systems more profitable, or giving more tools to patients who already have access, it will widen the gaps it claims to close. The technology will compound existing advantage.
But aimed deliberately at the people healthcare routinely misses, AI becomes something different — a tool for equity at scale.
Dr. Chokshi put the scale of the problem plainly: there are 100 million people in the United States without regular access to a doctor. They’re absent from care because of cost, distrust, immigration concerns, logistical barriers, or earlier experiences of being failed by the system.
Reaching them isn’t a technology problem first. It’s a trust problem.
Why Relationships Still Drive Outcomes

Dr. Chokshi draws from his clinical work at Bellevue Hospital with patients experiencing homelessness. When a patient walks in who hasn’t seen a doctor in years, the electronic health record may be full of overdue alerts and flagged conditions.
But the actual clinical priority in that moment is more fundamental.
“My job as a physician to so many of my patients is simply to forge enough of a relationship with them, to have them trust me enough, to come back for a second visit.”
That’s the frame healthcare leaders need when evaluating AI tools. The question isn’t just whether a tool increases throughput or reduces documentation time. It’s whether it creates more space for the human work of care — or adds another layer of friction on top of it.
AI that reclaims time for clinicians, supports community health workers, and reduces administrative waste can do more for health outcomes than AI that simply accelerates paperwork. Dr. Chokshi is explicit: productivity shouldn’t mean doing more to patients. It should mean eliminating the complexity and waste that gets in the way of actual care.
“Everything that is good, everything that works in our health system is because it is oriented around a human relationship. So that’s the starting point.”
The Patients Healthcare Doesn’t See

There’s a phrase Dr. Chokshi uses that reframes how you think about clinical work entirely: “the patients we do not see.”
When clinicians make rounds or see patients in clinic, they’re working with the people who made it through the door. But from a public health perspective, those are only the visible cases. The real challenge is the population that never crosses the threshold — people who are sick, who would benefit from proven interventions, and who the system has no reliable mechanism to reach.
AI’s most meaningful contribution to healthcare may not be in the clinic at all. It may be in the gap between the clinic and the community — identifying who’s missing, understanding why, and building the connective tissue that brings proven care to people before crisis forces their hand.
What This Means for How You Evaluate AI Tools

If you’re a healthcare leader, operator, or decision-maker assessing AI tools, Dr. Chokshi’s framework gives you a sharper filter.
Ask not just what a tool discovers or predicts, but what it delivers. Does it help identify patients who are falling through the cracks? Does it reduce the friction between diagnosis and completed treatment? Does it support the workers — community health workers, navigators, care coordinators — who do the relationship-intensive work of reaching underserved populations?
Tools that answer yes to those questions are addressing healthcare’s most persistent failure. Tools that don’t are optimizing the margins of a system that already works for people who already have access.
The Real Breakthrough

The next wave of AI in healthcare will produce genuine discoveries. Some of them will be remarkable. But the breakthrough Dr. Chokshi is pointing to is quieter and more urgent: can AI help medicine act on what it already knows?
Can it find the patient with undiagnosed hepatitis C? Help someone complete HIV prevention treatment? Reduce the waiting and paperwork that consume patients’ lives? Bring proven care to people who never reach the clinic door?
That’s not a lesser ambition. It’s a harder one — and arguably a more important one.
As Dr. Chokshi framed it: “How do we get from breakthrough to follow-through to realize the actual health benefit of the transformative technologies that we already have in our midst?”
The tools exist. The science exists. The gap between them and the patients who need them most is where AI’s real work begins.




Comments (0) No comments yet
Want to join this discussion? Login or Register.
No comments yet. Be the first to share your thoughts!