

The 191-Task Problem

A decade-old research paper recently resurfaced on LinkedIn, shared by Dr. Paulius Mui, and it stopped a lot of people in their tracks.
Researchers observed 30 primary care physicians across 17 clinics in Wisconsin and Iowa — urban and rural, academic and community, EHR and paper-based. They watched real patient visits. They recorded every single task. They coded the data systematically.
The result? 191 distinct tasks in a single routine clinical encounter.
Twelve major categories. 189 subtasks. Tasks ranging from gathering a chief complaint to logging into the EHR to answering a page mid-visit to reviewing scratch paper notes. Something that looks simple from a distance is, on the ground, extraordinarily complex.
That gap — between how workflows look from above and how they actually run — is the core reason most healthcare AI tools miss the mark.
The Bird’s-Eye vs. Mouse-Eye Problem

Think about it this way.
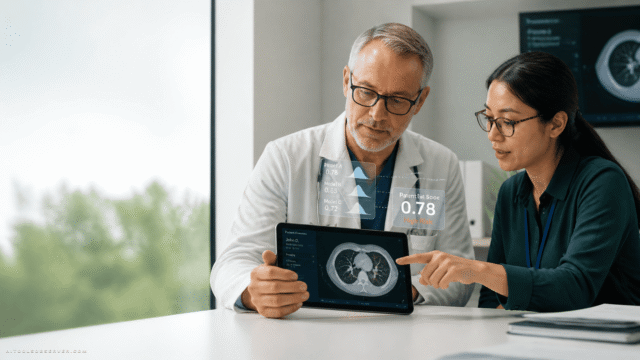
The bird’s-eye view is what most AI vendors operate from. Patient arrives. Vitals are taken. Physician enters. History is gathered. Exam is performed. Plan is discussed. Patient leaves. Clean. Linear. Logical.
The mouse-eye view is what actually happens. The patient hands an insurance card to the front desk. The MA places a blood pressure cuff, records vitals on paper, then logs into the EHR to update the chart. The physician turns back and forth between the patient and a computer screen mounted on the wall — because in most exam rooms, the monitor faces away from the patient. Sometimes the physician ends up talking to the computer instead of the patient.
Unless you’re physically in that room, you would never design around that detail. You wouldn’t even know it existed.
This is the hawk-and-mouse dynamic. The hawk sees the mouse moving through the grass. But the mouse is slipping on gravel, gnawing through tall grass, dropping into divots the hawk can’t see from above. Most AI builders are the hawk. Physicians are the mouse. And the tools being dropped into clinical workflows are landing in terrain the builders never mapped.
Why This Matters Right Now

We’re in the middle of a full-scale AI implementation wave in healthcare. Every health system is evaluating tools. Every vendor is promising efficiency gains.
But most of these tools are built on assumptions:
- That physicians have time to review AI-generated summaries
- That EHR interfaces are intuitive enough to work alongside new software
- That workflows are linear and predictable
- That the physician is sitting at a desk — not standing in a hallway with a faxed chart in one hand and a phone in the other
Those assumptions are wrong. And when the tool hits the real workflow, it doesn’t save time. It creates new clicks, new handoffs, new cognitive load. It adds to the 191 tasks instead of reducing them.
This isn’t a technology failure. It’s a workflow mapping failure.
What Ground-Level Workflow Analysis Actually Looks Like

Before medical school, Jared Dashevsky — internal medicine physician, incoming pulmonary and critical care fellow at Mount Sinai, and founder of Healthcare Huddle — worked on an automated waitlist solution for outpatient practices. He and a colleague didn’t just interview front desk staff. They went to physician practices in the Bethlehem area and watched.
They observed how staff moved their mouse between pages. Where they got stuck. What workarounds they’d invented. From that, they built detailed process maps — both high-level and granular.
That’s the gold standard. Not interviews. Not surveys. Shadowing.
Interviews miss nuance. People describe their workflows the way they think they work, not the way they actually do. Shadowing reveals the workarounds, the inefficiencies, the small frictions that compound into major bottlenecks — the details that never make it into a verbal description.
The payoff is real. Granular workflow maps can be iterated on, timed, and stress-tested. You can find the actual bottlenecks. You can identify the real problem your tool should solve — not the problem you assumed existed from 100 feet up.
How to Evaluate Healthcare AI Tools the Right Way

If you’re a clinical leader, practice manager, or health system evaluator being pitched AI tools right now, here’s what you need to demand before signing anything.
Ask if they’ve mapped your actual workflow
Have they shadowed your physicians? Have they timed tasks? Do they know where your specific bottlenecks are — not just the generic ones from a whitepaper?
Ask how the tool integrates at the task level
Which of those 191 tasks does it replace? Which does it add? Where does it create new handoffs? How many additional clicks does it require per encounter?
Ask what happens when it breaks the workflow
What’s the fallback when the AI is wrong? How long does it take a physician to override it? How much training is required before the tool stops slowing people down?
Ask for evidence from comparable settings
A tool that works in a large academic medical center may be completely wrong for a rural community practice. Context matters. Workflow context matters even more.
If a vendor can’t answer these questions with specifics, they’re operating from the hawk’s perspective. And you’re the one on the ground who will absorb the consequences.
The Real Adoption Gap in Healthcare AI

The conversation around healthcare AI adoption tends to focus on regulation, reimbursement, and physician resistance. Those are real barriers.
But the deeper, less-discussed barrier is this: most tools are not built for the workflow they’re supposed to improve.
They’re built for a cleaner, simpler version of that workflow — one that exists in pitch decks and product demos but not in actual exam rooms. When the tool meets reality, the friction is immediate. Physicians work around it. Adoption stalls. The health system moves on to the next vendor.
The paper that mapped 191 tasks was written during the EHR rollout era — precisely to help clinics plan intelligently before implementing major changes. The lesson was clear then. It’s still being ignored now.
The Takeaway

Workflows are not simple. They never were.
The AI tools that will actually stick in clinical settings — the ones that reduce burnout, improve documentation, and genuinely support physician decision-making — will be the ones built by teams who did the ground-level work first. Who shadowed. Who timed. Who mapped every nook and cranny before writing a single line of code.
For everyone else evaluating tools right now: the right question isn’t “does this AI work?” It’s “does this AI work in my workflow?” Those are two very different questions. And only one of them will tell you whether you’re about to solve a problem or create 20 new ones.



Comments (0) No comments yet
Want to join this discussion? Login or Register.
No comments yet. Be the first to share your thoughts!