

The Problem No One Has Solved Yet
Doctor shortages aren’t a developing-world footnote. They’re a structural crisis reshaping how cardiac care can realistically be delivered.
Pakistan has fewer than one physician per 1,000 people. Sub-Saharan Africa averaged around 0.2 per 1,000 in 2022, according to World Bank data. Even in countries with stronger health systems, specialist follow-up after cardiac events is inconsistent, delayed, or simply unavailable outside major urban centers.
The math is brutal: you can’t train enough cardiologists fast enough to meet demand. So the question becomes — what can extend the reach of the ones you have?
A Post-Discharge Monitoring System at Fuwai Hospital

Fuwai Hospital in Beijing is one of the world’s largest cardiovascular centers. A team there, working with cardiologist Wu Yongjian, has been designing a system to keep patients visible to clinicians after they go home.
The model combines inpatient records with follow-up data from questionnaires and wearable devices. Patients interact through mobile tools. The system generates risk scores and escalation alerts between hospital visits — essentially a continuous signal where there was previously silence.
The broader ambition is to encode specialist clinical expertise into disease-specific AI models capable of supporting long-term patient management at scale. A multi-centre study is underway to gather clinical evidence, though details haven’t yet been independently verified in public trial registries. Promising, but still in motion.
ECGFounder — A Foundation Model Built on 10 Million ECGs

At Peking University, researcher Hong Shenda’s group took a different angle: the device and the model together.
They developed ECGFounder, an ECG foundation model published in NEJM AI in 2025. It was trained on more than 10.7 million ECGs from approximately 1.8 million subjects, spanning 150 label categories. Crucially, it works on single-lead readings — not just standard 12-lead clinical ECGs — which makes it relevant to mobile and wearable contexts.
The companion hardware is deliberately simple. A user presses two fingers against a compact device, waits about 30 seconds, and gets a single-lead ECG reading through a mobile interface. No clinic required. No appointment needed.
That’s the point. The goal isn’t to replicate a hospital cardiology suite. It’s to create a meaningful signal where there currently is none.
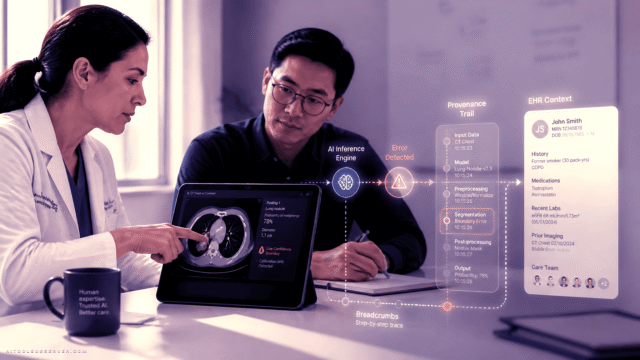
Traceable AI, Not Autonomous Diagnosis
For any of this to work in practice, clinicians need to trust the alerts they receive. That’s where Yidu Tech, a Chinese clinical AI company, offers a relevant design principle.
Their evidence-based medicine agent links every conclusion to its underlying guideline or literature source. Doctors can verify the original material before acting. It’s a small but significant architectural choice — and it reflects a broader theme emerging from China’s medical AI community: the goal is traceable support, not autonomous decision-making.
AI raises the flag. The doctor still makes the call.
The Structural Walls That Remain
None of this works without data flowing freely — and right now, it mostly doesn’t.
Patient records, wearable device data, and insurance information typically sit in separate systems with no clean integration. The Fuwai team acknowledged this directly: their long-term vision requires inpatient data, home monitoring data, and insurance data to be connected. At the moment, that connectivity is a goal, not a given.
There’s also the accountability question. Continuous monitoring only works if the AI knows when to hand a decision back to a human — and if it’s unambiguous who bears responsibility when it doesn’t. Regulatory frameworks for open-ended medical AI systems remain unsettled in China and most other markets.
And then there’s the gap between a compelling research demo and a validated clinical tool. That gap is where most medical AI projects face their hardest test. Follow-on work from Hong’s team is exploring cardiac biological ageing and future disease-risk prediction — genuinely exciting territory, but still firmly in the research phase.
Why This Matters Beyond China
The use case China is building for isn’t uniquely Chinese.
In Pakistan, parts of Africa, and underserved regions globally, the same structural problem applies: too few specialists, too little follow-up capacity, too many patients discharged into a monitoring void. AI-assisted ECG tools and phone-based follow-up systems — if properly validated — could help health workers identify higher-risk patients earlier, without requiring a cardiologist in the room.
The model isn’t about replacing cardiologists. It’s about using their expertise more efficiently — encoding it into systems that can triage, flag, and support routine follow-up closer to where patients actually live.
But the conditions for success are non-negotiable: local clinical validation, affordable devices, clean data pipelines, and clear protocols for who responds when the software raises an alert. Without those, even the best AI model stays a hospital pilot.
The Takeaway
China’s AI ECG experiments are early, imperfect, and still accumulating evidence. But they’re pointing at something real: the possibility of extending specialist-level cardiac monitoring beyond hospital walls, into the daily lives of patients who currently disappear from clinical view the moment they’re discharged.
For health systems stretched thin by doctor shortages, that’s not a nice-to-have. It’s a structural necessity.
The tools are getting there. The harder work — data integration, regulatory clarity, clinical trust — is still catching up. Watch this space closely. The gap between pilot and scale is exactly where the most important decisions get made.


Comments (0) No comments yet
Want to join this discussion? Login or Register.
No comments yet. Be the first to share your thoughts!