

The Technology Isn’t the Problem

That’s the uncomfortable truth buried inside AI For Health: Converting Momentum Into Muscle — a report from Singapore’s Health Empowered by AI Launchpad, shaped by more than 60 health leaders and clinicians in 2025.
The barriers aren’t algorithms. They’re people, processes, and the quiet friction of getting new tools to actually stick inside large, complex organisations.
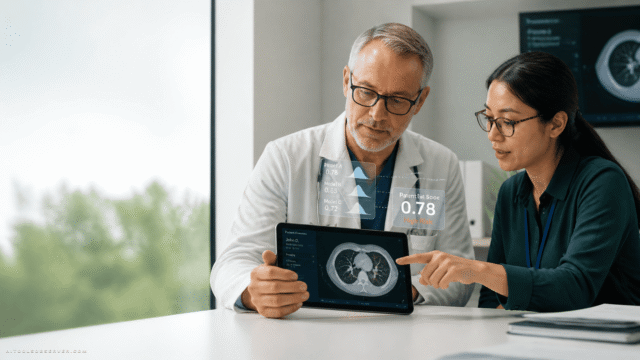
Walk into any Singapore hospital today and you’ll find AI running somewhere — a risk-scoring model, a scheduling tool, a chatbot fielding routine queries. What you’ll find less often is evidence that any of it changed how care actually feels for patients or staff.
That gap between “deployed” and “working” is the whole problem.
The Coordination Gap

Good ideas start in one team and stay there. A neighbouring department builds the same thing six months later, unaware it already exists. Learning doesn’t spread. The result is a health system running hundreds of small experiments with very little lasting change.
It’s not a technology failure. It’s an organisational one.
The Reality Gap

A tool that performs beautifully in a demo often struggles at 2am on a busy ward. It may not fit how staff actually work under pressure. Worse, it may add a step rather than remove one — and in healthcare, asking an already-stretched nurse to do something extra is a fast path to quiet abandonment.
The Trust Gap

Staff hesitation isn’t irrational. In healthcare, scepticism about a new system is often just good clinical instinct wearing a different hat. Without clear guidance, honest training, and a culture where raising concerns is welcomed rather than managed away, some staff forge ahead confidently while others get quietly left behind.
Governance: Fuel or Friction?

Healthcare takes safety seriously. That’s non-negotiable. But there’s a meaningful difference between oversight that protects patients and oversight that buries promising ideas in process.
Traditional approval systems were built for stable technologies — devices that behave the same way every time. AI doesn’t work like that. It learns. It drifts. It performs differently depending on who’s using it and where.
Applying the same lengthy sign-off process to an administrative chatbot as to a cancer-detection system doesn’t add safety. It just adds delay.
One participant in the 2025 discussions put it cleanly: Governance should fuel confidence, not restrain it. That framing matters. The goal isn’t less oversight — it’s smarter oversight, calibrated to actual risk.
What’s Actually Working
The teams making real progress share one habit: they start with the problem, not the technology.
Documentation Relief at Woodlands Hospital

Medical social workers were drowning in notes. An AI transcription tool now listens during consultations, drafts the notes, and gets out of the way. Documentation time dropped by more than 40%. That’s not a marginal improvement — it’s hours returned to patient care every single day.
Smarter Scheduling at NHG Health

Building nursing rosters is tedious, time-consuming, and surprisingly consequential for staff retention. An AI scheduling system cut roster-building time by 83%, improved retention, and freed up resources equivalent to nearly 60 full-time positions annually. The nurses didn’t get replaced. They got their time back.
NHG HealthBot on WhatsApp

Patient support, now available on the platform people already use. On track to handle nearly a quarter of routine health inquiries — reducing pressure on call centres while genuinely improving access for patients who’d otherwise be on hold.
None of these succeeded because the technology was extraordinary. They succeeded because someone identified a real frustration, worked with frontline staff to understand it, and built around their needs — not around what was technically impressive.
Singapore’s Structural Advantage (and What It Won’t Do Automatically)

Singapore is unusually well-positioned here. A relatively coordinated public health system. Strong digital infrastructure. A clear national interest in making healthcare sustainable as the population ages.
But advantages don’t translate automatically.
The harder work is in the less visible foundations:
- Shared digital infrastructure across different parts of the health system
- Risk-calibrated approval processes that move fast on low-stakes tools and carefully on high-stakes ones
- Training that reaches everyone — not just the tech-savvy few
- Honest evaluation that asks whether patients and staff are genuinely better off, not just whether the project shipped on time
And perhaps most importantly: a willingness to talk openly about what hasn’t worked. Health systems that make real progress treat a failed deployment as a lesson, not something to quietly shelve.
The Metric That Actually Matters

Excitement about AI is easy. Singapore has plenty of it, and much of it is justified.
But excitement alone won’t change what it feels like to wait three weeks for an appointment. It won’t prevent a nurse working a double shift. It won’t give back the hours clinicians lose every day to documentation instead of patients.
What will change those things is quieter, harder work — building organisations that can adopt new tools safely, learn from experience, and improve steadily over time.
The goal isn’t to build the most algorithms. It’s to become the place where AI in healthcare is implemented well — safely, equitably, and at scale.
The goal isn’t to build the most algorithms. It’s to become the place where AI in healthcare is implemented well — safely, equitably, and at scale.
That small word, implemented, carries everything.




Comments (0) No comments yet
Want to join this discussion? Login or Register.
No comments yet. Be the first to share your thoughts!