
The Problem With “We Know Best”
Healthcare AI has a trust problem. Not a capability problem — a trust problem.
Clinicians build tools optimized for efficiency. Engineers optimize for accuracy. And somewhere in that pipeline, the person actually lying in the hospital bed gets forgotten as a stakeholder.
Stanford noticed this gap. The fix wasn’t more data. It was more listening.
Meet the Panel

Eric Gries didn’t apply for a clinical trial. He was handpicked.
Gries served as caregiver for his wife through a left ventricular assist device (LVAD) and a heart transplant — then did it again for his brother-in-law. That’s not a patient story. That’s a masterclass in navigating high-stakes medical systems under pressure.
Stanford wants people like him in the room when new AI tools are being evaluated. People who’ve lived inside the complexity these tools are supposed to simplify.
The patient panel isn’t a focus group. It’s a structured feedback mechanism built into the pre-launch workflow.
The Setup
Stanford identifies patients and caregivers with relevant experience — not just any willing volunteer, but people whose backgrounds map to the clinical context of the tool being reviewed.
Gries, for example, is exactly the kind of user who would interact with cardiac care AI. His feedback isn’t hypothetical. It’s grounded.
The Feedback Loop

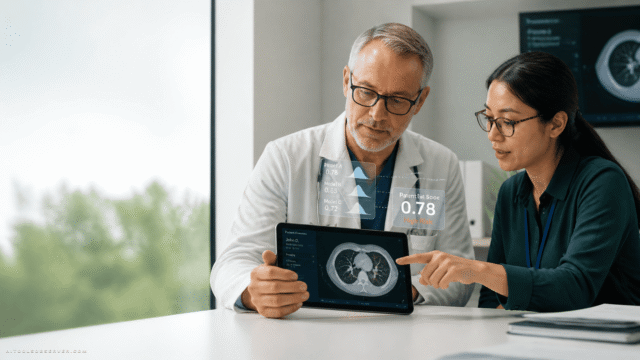
Panelists review tools, ask questions, flag concerns, and surface blind spots that clinical teams often miss. Things like: Does this interface make sense when you’re exhausted and scared? Or: What happens when the AI is wrong and the patient notices first?
These aren’t edge cases. In real hospital environments, they’re Tuesday.
The Output
Feedback shapes the tool before deployment — not as a checkbox, but as a genuine input into design and governance decisions. The goal is AI that patients can trust, not just AI that clinicians can defend.
Why This Is a Case Study Worth Watching

Stanford isn’t the first institution to talk about human-centered AI. But running a standing patient panel — with real caregivers, real stakes, and real influence over launch decisions — is a meaningful operational commitment.
It’s also a replicable model. You don’t need Stanford’s budget to ask patients what they think before you ship.
Limitations to Note
Patient panels are only as good as their composition. If the panel skews toward highly educated, English-speaking, tech-comfortable participants, the feedback will too.
There’s also the question of scope. A panel can catch usability issues and surface distrust. It can’t fully simulate the chaos of a real clinical environment at 2 a.m.
And like any governance mechanism, it only works if the teams building the tools actually listen — not just collect responses and move on.
The Takeaway

The computer mouse was invented at Stanford. So was Google. The patient panel won’t make headlines the same way.
But in a field where AI tools routinely launch without meaningful input from the people they’re supposed to help, asking a heart transplant caregiver what he thinks before you go live might be the most important innovation on that campus right now.
Build fast. But ask first.



Comments (0) No comments yet
Want to join this discussion? Login or Register.
No comments yet. Be the first to share your thoughts!