

The Trap Isn’t Technical. It’s Structural.

Most people assume a failed AI rollout means the model underperformed. Usually, that’s not it.
The pilot ran in one department, leaned on one clinical champion, depended on one vendor integration, and survived on one favorable budget cycle. When the organization reaches for scale, it discovers that nobody owns the model, nobody can explain whether the data feed is static or dynamic, and governance is reviewing the tool after operational decisions have already been made.
That’s the pilot trap. It looks like a technology problem. It’s actually an operating model problem.
Hospitals Already Know How to Govern High-Risk Systems
This is the part that often gets missed in the AI conversation.
Health systems govern medications, medical devices, infection control, clinical workflows, and patient privacy — all simultaneously, all at scale. They’re not new to complexity or risk. What’s new is that AI touches all of those domains at once.
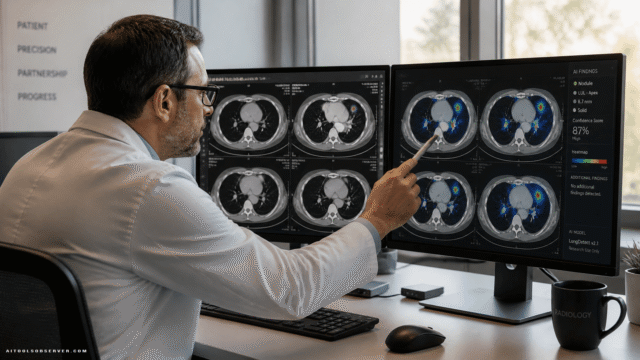
A single clinical model might pull from EHR data, trigger patient safety alerts, reshape nursing workflows, generate billing outputs, and sit on a vendor architecture that security and compliance teams haven’t fully reviewed. Treating that as a standalone innovation project misses how hospitals actually operate.
The Questions Governance Must Answer Before Production

A useful governance model doesn’t wait for something to go wrong. It answers operational questions before a tool goes live.
Things like:
- What data does the model rely on, and how is that feed monitored?
- Which clinical workflow does the AI influence?
- Who is the named technical owner?
- What risk tier does this tool fall into?
- What triggers a review, a pause, or a full stop?
- Which governing body has authority to scale, modify, or remove it?
These aren’t bureaucratic speed bumps. They’re the conditions that determine whether an AI tool can safely move from proof-of-concept to enterprise infrastructure.
An AI Committee Isn’t Enough
Many health systems responded to AI risk by forming an AI committee. Reasonable instinct. Insufficient outcome.
A standalone committee rarely has authority over clinical operations, capital planning, EHR change management, vendor procurement, or quality and safety reviews. It can review an AI tool. It can’t govern the decisions that make AI operational.
The more practical approach is routing — integrating AI governance into the decision-making bodies that already run the hospital.
What Routing Actually Looks Like
A deterioration model belongs with quality, patient safety, nursing, and clinical operations. Revenue cycle automation belongs with finance, compliance, and IT leadership. Vendor AI belongs in procurement, legal, privacy, and enterprise architecture review. Medication-related AI goes through pharmacy and therapeutics.
The central AI governance function still matters. But it needs a realistic way to operate inside the hospital’s existing structure — not parallel to it.
The Four Layers That Actually Enable Scale
There’s a practical roadmap here, and the sequence matters more than the components.
Governance and accountability comes first. Without it, everything downstream is performative.
Stable data pipelines come second. Without visibility into what the model is consuming, governance has nothing to act on.
Shared infrastructure and model architecture come third. Without this, every new AI tool becomes its own expensive, one-off maintenance burden.
Clinical adoption and dynamic governance come last. Without the first three layers, adoption becomes trust without surveillance — and that’s where things get dangerous.
Governance without data visibility is theater. Data pipelines without shared infrastructure are expensive. Infrastructure without adoption is sunk cost. Adoption without governance is a liability waiting to surface.
The Real Differentiator Isn’t More Pilots
The health systems that scale AI won’t necessarily be the ones with the most impressive pilots. They’ll be the ones that turned their pilots into governed, supported, trusted operating capabilities.
A pilot can survive on sponsor energy and local workarounds. A production AI stack requires authority, visibility, and ownership — the same things that make any other high-stakes hospital system function.
The goal isn’t to slow innovation. It’s to make innovation repeatable.
That’s a meaningful distinction. And it’s the one most organizations are still learning to make.


Comments (0) No comments yet
Want to join this discussion? Login or Register.
No comments yet. Be the first to share your thoughts!